
When our children are struggling in some way, we usually start with some basic adjustments: talk to their teacher, tweak sleep/food/activity schedules, talk with them directly, and wait to see if it’s a passing phase. When these first-level supports don’t work, the next steps often involve formal evaluation of some kind. We’re going to walk you through the kinds of evaluations you might consider and what to do with that whopping report when you receive it, so you can be a strong advocate for your child.
Common evaluations for children with developmental and/or learning difficulties include:
Speech-Language Evaluation – Completed by a Speech Language Pathologist (SLP). Thorough assessment of communication skills and functions, including speech production (speech sounds, voice, fluency), receptive language, expressive communication, social-pragmatics, play development (for young children), and language processing (for older children).
Occupational Therapy (OT) Evaluation – Completed by an Occupational Therapist (OT). An assessment of how a child performs daily activities and processes sensory input, especially related to fine motor skills, sensory processing, self-care skills, feeding, motor coordination, and regulation.
Physical Therapy (PT) Evaluation – completed by a Physical Therapist (PT). An evaluation of large muscle movement and physical functioning, including gross motor skills (walking, running, balance), strength, coordination, posture, and mobility.
Educational Evaluation (aka School-Based IEP Evaluation) – Completed by multidisciplinary school team (SLP, school psychologist, special educator, OT, etc.). A legally mandated evaluation (under IDEA) to determine eligibility for special education services and supports that includes assessment of academic performance, classroom behavior, communication, and functional skills in school.
Neuropsychological Evaluation – Completed by a Clinical Neuropsychologist. A deep, integrative assessment that examines how a child’s brain functioning impacts thinking, learning, behavior, and emotional regulation. Often used for complex profiles (e.g., giftedness, ADHD, autism, learning disabilities, dyslexia).
Psychological Evaluation – Completed by a Clinical Psychologist or School Psychologist. An evaluation focused on emotional, behavioral, and mental health functioning, often used to clarify diagnoses like anxiety, depression, or behavioral disorders. This sometimes includes assessment of cognitive abilities (basic IQ testing).
Psychoeducational Evaluation – Completed by a Clinical Psychologist or School Psychologist. An evaluation that compares a child’s cognitive abilities (including IQ) to their academic performance (reading, writing, math) to identify learning strengths, difficulties, and educational needs.
Developmental Evaluation – Completed by Developmental Pediatrician or multidisciplinary team. A broad screening or diagnostic assessment of a young child’s developmental milestones (including communication, motor, social-emotional, and adaptive/self-help) and overall developmental trajectory.
Autism Evaluation – Completed by Psychologist, Neuropsychologist, Developmental Pediatrician, or multidisciplinary team. A specialized diagnostic evaluation for Autism Spectrum Disorder, often using standardized tools (e.g., structured observations and caregiver interviews) to assess social communication, restricted/repetitive behaviors, play skills, and sensory processing.
Behavioral Evaluation (aka Functional Behavioral Assessment – FBA) – Completed by a Psychologist, Behavior Specialist, or Board Certified Behavior Analyst (BCBA). A systematic process for identifying the purpose a behavior serves, including the purpose/function of the behavior, triggers and consequences, and patterns across environments.
Whew! That’s a lot of options. After doing your research and consulting with your child’s pediatrician, you’ve determined which tests your child needs, scheduled the evaluation, and completed the testing session(s). A few weeks later, you get THE REPORT. Hopefully, the evaluator(s) will provide you with a chance to review the results together, ask questions, and make a support plan. Sometimes, all you get is the report. And in either case, you’re probably going to have information and emotion overload. Here are some suggestions about how to approach and process your child’s new evaluation report.
Where to Start
Often, these kinds of reports are long (sometimes very long!). It can be a lot to take in, especially when the report is full of jargony words that you might not completely understand. Proverbial wisdom applies here: “How do you eat an elephant? One bite at a time.”
An evaluation report should be approached in steps. And contrary to convention, it’s not usually the best idea to start at the beginning. An evaluation report will typically have the following sections.
Presenting Concerns: Why the child is being referred for an evaluation.
History / Development: Includes birth, health, family, and developmental background.
Initial / Behavioral Impressions: The testing environment and how the child participated / engaged.
Tests Administered: A list of the tests and subtests used to assess the child. The scores for each test might be listed in this section, within each area, and/or included in a score sheet at the end.
Results: A discussion of the child’s performance on formal and informal assessments, usually organized by discipline (for multidisciplinary reports) and area. For communication, the areas usually include receptive language, expressive language, speech production, and social skills as a core with additional areas when appropriate. This section will reference scores and the detailed examination of skills from a variety of tests.
Summary: A broad interpretation of the Big Picture with any relevant diagnoses.
Recommendations: The next steps that will best support the child.
To start your review of the evaluation report, get a highlighter (for the parts that really jump out at you) and pen (for jotting notes and questions in the margins). Settle into a comfortable seated space for some focused reading when you have a good chunk of uninterrupted time. Take a deep breath and get started.
As a parent and as a professional, I usually skim the presenting concerns and then jump straight to the Summary. That Big Picture overview gives me the foundation of what I’m reading: What were the areas of strength? What areas were challenging? How does this affect the child’s everyday life? And are there any diagnoses that are being assigned based on the child’s performance?
As a parent, it might be helpful to take a break here after finishing the Summary. Get up, get a glass of water, take a walk, or even put the report aside for the day. I recommend reading the Summary a couple of times. Different elements will stand out in each reading, and you want to have a complete understanding of the overall results.
Once you’ve finished digesting the Summary, you might be feeling overwhelmed or anxious about what this means for your child. We’ll get to the emotional impact later, but for now, the next best section of the report to read is Recommendations. This should be a thorough list of supports for home, school, therapy, and/or additional referrals. Don’t spend too much time combing through this section yet; we’ll dig deeper into this later. For now, reading the Recommendations can offer some basic reassurance that there is a plan.
Now that you’ve read and processed the Summary and Recommendations, it’s time to go back to the beginning. You have the Big Picture in mind, and that helps you understand the nitty-gritty details. Read the History with an eye to accuracy, making sure that the evaluator reported background information correctly. Review the Initial / Behavioral Impressions to make sure that your child’s participation, behavior, communication, and description sound like them. If there are big discrepancies between who you know your child to be and the child described in the report, talk to the evaluator. While this doesn’t mean the results are wrong (after all, your child did perform in this way for that situation), the results may not be reflective of your child’s typical performance.
And finally, you’ll read the details about the tests and results.
Understanding Scores
Reading the list of Tests Administered might not make any sense, if you’re not familiar with the test and/or what it’s evaluating. You don’t necessarily need to understand the tests if the evaluator explains the test and, more importantly, what your child showed on the test. If you want more information about the tests listed, it’s always a good idea to talk to the evaluator.
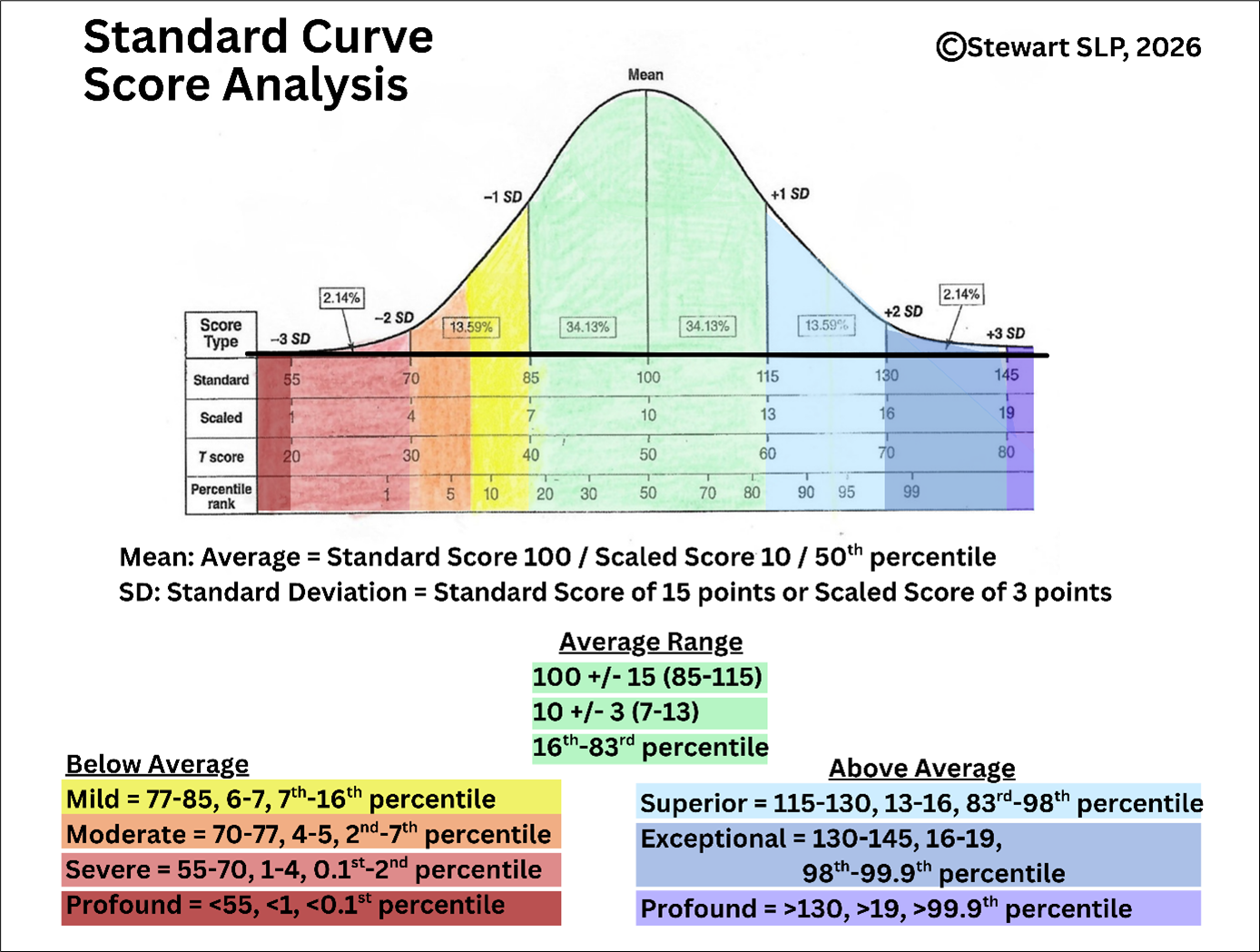
The Results section should be organized by skill/learning/domain area, since that approach groups information about functional performance together. However, depending on the context and evaluator, results may be organized by test. The Results section will reference scores and performance on formal and informal tests. Scores are usually based on a statistical analysis of a normed sample, which simply means that a bunch of people took this test when it was being developed, and the scores were analyzed into a standard curve that your child is being compared against. Below is a color-coded graphic of a standard curve with information about the following metrics:
Mean: Exact average score
Standard Deviation (SD): Very simply, this reflects how the data points from the norming sample cluster around the mean; it tells us how common it is for people to perform within a given range. The average range is comprised of all the scores within 1 standard deviation. For example, tests with a mean of 100 and a SD of 15 yields an average range of 100 +/- 15, meaning that the average range is 85-115. Scores between 1 & 2 SDs are less common (below or above average). Scores between 2 & 3 SDs are very uncommon (very below or very above average). And scores outside of 3 SDs are extremely rare.
Standard Score: The score your child earned on a test with a mean of 100.
Scale Score: The score your child earned on a test with a mean of 10.
Percentiles: The percent of people your child did better than. For example, the 50th percentile (exact average) means the child did better than 50 percent of children their age. The 16th percentile means the child did better than 16 percent of children their age. Percentile is a comparison metric to the general population; it is NOT percentage of accuracy.
Sometimes, scores are presented with a metric that is different from a standard curve. The most common examples include:
Criterion-Referenced: the child did or did not meet the criteria for a significant result in a given domain.
Adjusted Curves: the test’s norming sample does not fall on the standard curve, so scores will have a different average and standard deviation
Grade or Age Equivalents: a student's performance is compared to the median of specific grade levels or ages. In other words, the grade or age at which the child’s score is most common.
Take a look at the score table of your child’s evaluation report (if included) to get a sense about where your child’s scores fall. If there isn’t a score table, you can ask for one or try to keep track of scores within each narrative area. Look for the following patterns:
See if the scores fall within a similar range (e.g., mostly average, mostly mildly below average, etc.).
See if certain areas are stronger or weaker than others.
See if there are outliers – scores that fall much higher or lower than your child’s other scores.
In addition to scores, the Results section will include informal testing results & impressions along with brief discussion of the expected functional impact these scores are likely to have on the child’s academic, social, and functional life. Most of that interpretation of impact will be in the Summary, but some will be in Results as well. And that leads us back to the Summary. Once you’ve finished reading the Results, re-read the Summary again. Hopefully, the details from the Results will fill in any initial questions you had from your first readings of the Summary. And if not, it’s always a good idea to ask the evaluator.
The Diagnosis
Now, let’s get into the emotional element we touched on earlier. If the evaluation assigned a diagnosis (or two, three, or more) to your child, or even if the evaluation didn’t assign a diagnosis, it is completely normal for you to have some feelings about that. You might have lots of different feelings at the same time. And whatever you’re feeling, it’s OK. I promise. You are not the first parent to have any/all of these feelings, and you won’t be the last.
Relief: Sometimes, the results can feel validating. You suspected something, and the results can confirm your suspicions.
Fear: You might feel worried, anxious, or scared about what this diagnosis means for your child.
Confusion: You might feel like the information doesn’t make sense or that you don’t understand what the report is saying.
Overwhelmed: It’s a lot of information to process, and you might feel like you’re in the middle of a tornado.
Angry/Disappointed: You might feel like this diagnosis changes something about your child or that your child has failed to live up to your expectations or societal expectations.
Denial: You might not believe the results and/or diagnosis.
Step one: Be gentle with yourself. Take a breath. Give yourself some time to let the information settle. Talk to your partner, a therapist, a good friend, and/or journal. Practice the self-care routines that work best for you. Ground yourself.
Step two: Be gentle with your child. Your child is the exact same child they were before the evaluation. Nothing about your child has changed. What has changed is the information you now have about how your child functions in their world. You will love them just the same as you did before. And now, you might be able to help them better.
Step three: When you’re ready, go back to the Recommendations. This should be a thorough list of supports for home, school, therapy, and/or additional referrals. It should be individualized to the child’s profile and needs, and it should utilize the child’s strengths to support areas of challenge. If the Recommendations section feels light, ask the evaluator(s) for more. This is your roadmap for moving forward. And you will move forward. The evaluation has captured a snapshot of your child in one moment of time. They will continue learning and growing, and the recommendations can help you maximize their success. You need to feel secure that the roadmap presented in the Recommendations section is clear, even if it’s complicated.
Next Steps
The Recommendations should include a variety of suggestions that might include any, some, or all of the following (and maybe even more!):
Classroom Accommodations: Strategies that are implemented by the school team to support the child’s academic and social development at school. Contact your child’s teacher and/or school Special Education team to discuss the recommendations and get accommodations in place.
Home Strategies: Suggestions to improve the child’s overall functioning at home. Consult with your partner and/or co-parent to discuss if and how to implement these strategies.
Therapies: Individual and/or group therapy (SLP, OT, PT, psychology or counseling, play therapy, art therapy, music therapy, consulting, etc.) targeting particular areas of difficulty. Ask the evaluator and your child’s doctor for specific recommendations for providers. You might also check in with local friends and neighbors about who they have liked working with for their children. Remember that free public services are offered through your school district of residence for birth – 26 years. You might prefer school-based services, private services, or a combination of both.
Tutoring and/or Academic Intervention: If the evaluation indicated areas of academic difficulty, you may get recommendations for academic interventions from tutors and/or Special Education teachers at your child’s school.
Medication: Depending on the type of evaluation, you may see recommendations to consider medication trials. Consult with your child’s doctor and a pediatric psychiatrist to get guidance about this decision and the process.
Additional testing: If the evaluation identified an area of concern outside of the scope of that evaluation, there may be referrals to other specialists for further testing. For example, if an SLP noticed sensory regulation challenges during their communication evaluation, they might recommend pursuing an OT evaluation.
As you wrap up reviewing your child’s Evaluation Report, there are a couple of final important notes to consider:
You should feel empowered to follow up with the evaluator if you have any questions about the evaluation. If you still need more support understanding or processing the evaluation, consider reaching out to other trusted friends or professionals who are in related fields.
Testing is confidential. You are not obligated to share the results or report with anyone.
If you are unhappy or uncertain about the testing process, results, and/or report, it’s OK to consider getting a second opinion.
If your child is old enough and capable enough to be involved in discussions about their challenges, testing, goals, strategies, and supports, it’s important to include them. It’s their life, and they will feel better about themselves and their interventions if they have a say in the process.
Your child deserves whatever supports help them grow, and you deserve to understand what they need. You are your child’s strongest advocate. If you need help, reach out to us. Stewart SLP can help you understand your child’s report and find a good path forward.